Marfan Disease

Marfan syndrome (MFS) is an autosomal dominant connective tissue disorder and is caused by mutations in the gene coding for fibrillin-1 (FBN1). MFS is a typical example of a rare disease with a prevalence of <1 per 5,000 and a similar frequency in both sexes and in all countries and races. It is a severe, chronic, life-threatening disease with multiple organ involvement including the skeletal, ligamentous, occulo-facial, pulmonary, abdominal, neurological, and cardiovascular systems.
Cardiovascular complications
Cardiovascular complications, which involve the aorta and aortic valve, contribute most significantly to patient morbidity and mortality. It is well known that poor life expectancy in MFS is mainly triggered by cardiovascular complications such as acute aortic dissection or rupture. In most cases, aortic root dilatation is the predominant aortic manifestation.
To avoid acute aortic syndromes in MFS, prophylactic surgery of the aortic root should be performed when indicated according to current guidelines: irrespective of the presence and severity of aortic valve regurgitation, surgery is indicated in patients with Marfan syndrome who have aortic root disease with a maximum ascending aortic diameter of ≥50 mm (Class I, Level C evidence); moreover, surgery should be considered in patients with risk factors (family history of dissection, size increase 2 mm/year in repeated examinations) who have aortic root disease with a maximum ascending aortic diameter of ≥45 mm (Class IIa, Level C evidence).
Although composite-graft replacement with an aortic valve prosthesis as Bentall procedure remains the standard, most studies have shown excellent results using valve-sparing root replacement procedure such as the reimplantation technique or the remodeling technique.
Read more of Aortic Root Replacement here.
Also both techniques show good long-term results, the reimplantation technique well known as David procedure demonstrates higher freedom from significant long-term aortic insufficiency in Marfan syndrome because the aortic root and annulus are more stabilized. In contemporary practice, in experienced units, the mortality for elective surgery in these patients is under 1%; anticoagulation therapy is not required and valve-related complications are rare. According to current guidelines, valve-sparing procedure is now recommended in young patient (Class I, Level C evidence).
David procedure video
Mitral valve dysfunction
Mitral valve dysfunction is extremely common in young patients with Marfan syndrome. Although the majority of patients with Marfan syndrome who undergo elective aortic root replacement have a mitral valve prolapse, only 20% have a significant mitral regurgitation and a concomitant mitral valve procedure; In patients with mitral regurgitation grade ≤ 2 who do not undergo a concomitant mitral valve procedure, the short-term incidence of progressive mitral regurgitation is low and prophylactic mitral valve intervention is not justified. Patients with Marfan syndrome and mitral regurgitation have better survival with repair than with replacement; moreover survival and risk of reoperation for patients with Marfan syndrome were similar to those for patients with myxomatous mitral disease. These results support the use of mitral valve repair in patients with Marfan syndrome and moderate or severe mitral regurgitation.
Read more of Mitral Valve Repair here.
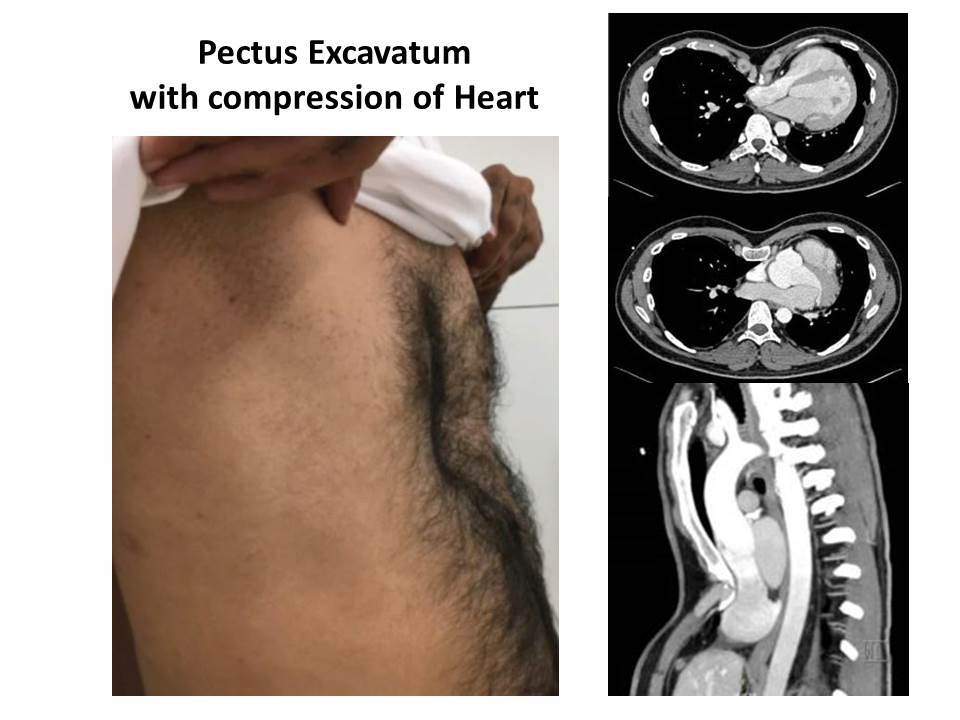
Pectus excavatum
Pectus excavatum is a commom chest wall malformation associated with cardiac abnormalities in Marfan syndrome. Pectus deformity is often associated with a shift of cardiac structures in the left thorax and/or their mechanical compression by the depressed chest wall.
When cardiac anomalies are associated and indication of their correction is mandatory, the surgical strategy is challenging. Single-stage correction of both lesions is currently the method of choice. Simultaneous cardiac and pectus deformity repair may be performed successfully with no added morbidity and excellent long-term results with regard to chest wall contours.
Marfan Disease Pectus Surgery with Mitral valve Repair and Aortic Root Replacement
Read this article for additional information on Marfan syndrome:
One-stage surgical repair of heart disease and pectus excavatum in Marfan syndrome [PDF, 985.61 KB]
It is imperative for all health care providers to understand the clinical features, progression, and management of Marfan syndrome to appropriately care for their patients. Ensuring regular follow-up and adherence to medical and surgical prophylaxis is essential to patient well-being. A multidisciplinary health care team is a means to maximize therapeutic success of patients with Marfan syndrome.